


















Abstract
Disposal of Bio-medical waste is a serious problem in India. Despite the existence of rules (Guidelines for Management of Healthcare Waste as per Biomedical Waste Management Rules, 2016) the waste is still not being disposed off properly. A rule of thumb for medical waste production in affluent countries seems to be 1kg per bed per 8-hour shift. India is all set to generate 775 tons per day of biomedical waste in 2022. Increased public concern has resulted in more regulations and court actions on a global scale. In India, to introduce a clean and safe technology Institute for Plasma Research (IPR), Technology Information Forecasting & Assessment Council (TIFAC) and Department of Science and Technology (DST), developed a plasma mediated process. In this technology extremely high temperature is produced using plasma torch in an oxygen starved environment which destroys bio-medical waste efficiently and in an environmentally friendly manner. Details of the plasma system technology are elaborated in the article.
Author

Prof John Pucadyil held the Meghnad Saha Chair for Plasma Science and Technology at Institute for Plasma Research, Gandhinagar, India. He established the Facilitation Centre for Industrial Plasma Technologies (FCIPT) to link the Institute with industry. Prof. John has 90 publications in international journals and holds 12 patents for plasma devices and plasma processes. His book “Plasma Sciences and the Creation of Wealth”, published by Tata McGraw-Hill in 2005, addresses a broad audience on the value addition through plasma-based technologies. The book has been translated into the Chinese language. His second book “Plasma Processes for Energy and Environment” was published by Lambert Publishers in November 2017.
Introduction
An international scandal involving a vast intra-European traffic in medical waste, originating from France and culminating in eventual redistribution in other European markets in the late 1980s, led to the resignation of the then French minister of health. As a result, the world was shocked to recognise the magnitude of the medical waste disposal problem. India is no stranger to such horror stories. Recycled syringes and quilts packed with used surgical cotton have a thriving market. Newspaper reports on rackets based on recycling medical waste back into the market abound. Photographs of hospital backyards filled with medical waste appear regularly. Pathogens of deadly diseases like hepatitis B find a ready and fertile breeding ground in the piles of undisposed medical waste. This is despite the existence of rules (Guidelines for Management of Healthcare Waste as per Biomedical Waste Management Rules, 2016) concerning the handling and remediation of biomedical waste.
The Medical Waste Problem
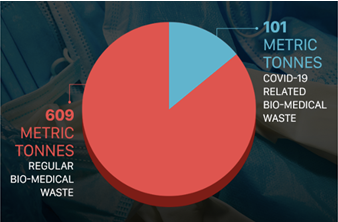
Public concern over the disposal and treatment of medical waste has resulted in increased regulations and court actions on a global scale. The fundamental reason is the phenomenal growth in the quantity of medical waste generated in the hospitals, attributed to the growing use of disposables as precautions against exposure to infectious diseases such as AIDS and the growth of medical and public health facilities. The recent COVID pandemic multiplied the medical waste problems many times. The generators include hospitals, clinics, and medical research facilities. A rule of thumb for medical waste production in affluent countries seems to be 1 kg per bed per 8-hour shift. India is all set to generate around 775 tons per day of biomedical waste in 2022, with current levels being 551 tons per day. United Nations Environment Programme (UNEP) study has estimated that due to the COVID pandemic, an increase of around 0.5 kg per bed per day of BMW is expected.
Conventional Remediation Techniques
Historically, landfilling was the most preferred means of disposal of medical waste. However, public opposition and positive correlation with groundwater contamination have resulted in this option steadily going out of favour. Burning the waste material in the open air can never be complete, with small quantities of many organic and chlorinated organic compounds and pathogens surviving and leading to the dispersal of dangerous diseases that can spread through the air. Therefore, incineration is the most popular method of medical waste disposal. About 85% of medical waste is incinerated, while only 6–15% is waste that requires special handling and disposal.
The fundamental problem of incineration is that combustion’s chemistry determines heat generation. Efficient combustion demands airflow far above the stoichiometric requirement. The very high flow rate generates airborne pollutants and limits the attainable temperature. As a result, the effectiveness of incineration, measured in terms of the destruction and removal efficiency, is low. In addition, the performance of the emissions control equipment to meet the stringent requirement of safe disposal is poor.
The Dioxin Problem
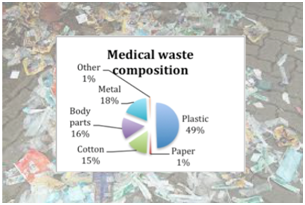
PVC (Polyvinyl Chloride) plastic, which contains chlorine, constitutes many disposable products used in health care. When PVC products burn, they serve as a primary source of chlorine for dioxin formation. “Dioxin” refers to a family of compounds that can form when chlorine combines with organic material in a reactive environment. Dioxins and related chlorinated organic compounds are potentially toxic substances that produce a remarkable variety of adverse effects in humans and animals at low doses. These compounds are persistent in the environment and accumulate in magnified concentrations as they move up the food chain, concentrating on breast milk. Dioxin is carcinogenic, interacting directly with DNA through a receptor-based mechanism.
The TIFAC initiative
In the late 1990s, the Technology Information Forecasting and Assessment Council (TIFAC) approached Institute for Plasma Research (IPR) to develop a Plasma Mediated process for medical waste destruction. With dramatic developments in high-temperature plasma sources, we thought we could apply plasma heat to highly toxic waste, and the final products can be harmless gases. The large flux of ultraviolet radiation in thermal plasma can dehydrogenate organic chlorine. The reactors were to process gaseous, liquid, and solid materials. Plasma-based medical waste treatment is highly complex since it must contend with extreme temperatures and a corrosion-prone environment. The process depends on complex pyrochemistry resulting in toxic and dangerous products.
Furthermore, it deals with high volume, low packing density waste with a non-standard composition comprising various plastics, organic materials, and liquids. As a result, compliance with environmental emission standards is complex. In addition, there are capital and operating cost constraints imposed by inferior competitor technologies. Being an internationally competitive technology with very high commercial stakes, critical information on many crucial aspects was not readily available. No peer group with expertise in this field existed in India for problem-solving consultations. Under a development programme with intense time pressure, many problems will have to be solved concurrently with development.
The Plasma Torch

The workhorse of plasma-based waste destruction technology is the plasma torch. Plasma torches are electrical discharge plasma sources with the plasma extracted as a jet through an opening in the electrode andout of the confines of the cathode-anode space. The arc column’s inherent thermal and electromagnetic instabilities are stabilised by forced gas flow along the current path. Interaction with a guiding wall or external magnetic fields also stabilises the plasma.
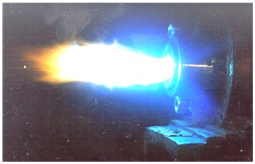
DC arc, RF and microwave plasma sources can be converted into plasma torches. Plasma temperatures can easily reach tens of thousands of degrees, and high enthalpy gas flows get generated in large volumes. The driver for developing plasma torches was the space race in the 1960s. Missiles re-entering the atmosphere create shock-ionised air plasma. Laboratory simulation of these conditions was necessary to develop materials capable of withstanding the searing heat of re-entry. Arc systems can generate re-entry conditions using clean, high enthalpy gases at high stagnation pressures. Many present-day plasma torches are derivatives of the plasma jet sources built for this application and now meet the need for intense heat sources for waste treatment.
Pyrolysis Process
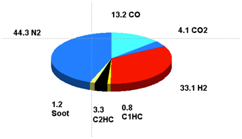
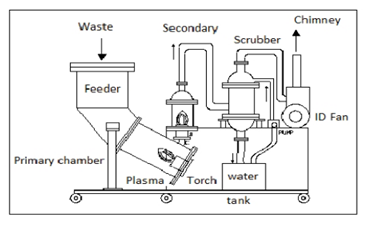
Pyrolysis is the thermal disintegration of carbonaceous material into fragments of compounds in an oxygen-starved environment. The presence of charged and excited species renders the plasma environment highly reactive, catalysing homogeneous and heterogeneous chemical reactions. When the process is optimised, the most likely compounds to form are methane, carbon monoxide, hydrogen, carbon dioxide, and water. The high temperature and high enthalpy inhibit the formation of hydrocarbons. The product gas is high in hydrogen and carbon monoxide, with traces of methane, acetylene, and ethylene; therefore, it can be combusted very efficiently, resulting in carbon dioxide, nitrogen and water vapour being the only gaseous exhaust to the atmosphere. The slag is a homogeneous, silico-metallic monolith with leachate toxicity levels orders of magnitude lower than current landfill regulations. Emission and leachate results convincingly demonstrate that plasma gasification is a far more environmentally friendly method of disposing waste than any competing technology. Plasma gasification provides more than a 95% volume reduction ratio of slag to input material. Other technologies offer an 80% reduction typically.
Prototypes
The prototype plant was built by Dr Ganesh Prasad (Plasma Physics) and Dr Sudhir Nema (Chemistry), both Scientists at FCIPT, using a conventional plasma torch and was installed at the Gujarat Cancer Research Hospital for field trials.Using the field experience, we built a series of prototypes to solve operational problems and improve reliability. We used an in-house developed graphite electrode plasma torch for ruggedness and energy efficiency. This used graphite electrodes with automated movement to keep plasma impedance constant.
A commercial version of a Plasma Reactor came after we installed the second field version at the Goa Medical College in 2000. Manohar Parrikar, the then Chief Minister of Goa, came to see the facility and complimented our team on the excellent engineering of the plant.
The Endogenous Gas Fed Plasma Torch
Conventional plasma torches require large gas throughput to stabilise the arc, resulting in product gas dilution and reduction in energy efficiency. We have innovated the graphite torch exploiting the gas generation in the pyrolysis of organic matter. An inline suction pump sucks the product gas and sends it through a filter to remove soot particles. It is then fed to the plasma torch. We had a 35 % gain in energy efficiency with this torch.It also increases electrode life by reducing the electrode erosion rate. We received a patent for the Endogenous Gas Feed concept in 2007.
Fields Trials and Regulatory Approval

After the successful trial of the system in the Goa Medical College, the Department of Science and Technology sponsored a programme of demonstration of this technology by installing several plasma systems all over the country, including one at the Shri Chitra Institute in Trivandrum. A large number of systems enabled extensive field trials of this technology. The technology was transferred to several manufacturers. About 1 KWh of power is required for 1 kg of waste. A 3 phase supply is adequate as the power source. A 25 KW unit is adequate for a 50 bed hospital.
The final battle that the development effort on pyrolysis technology had to fight was with the Regulatory Bureaucracy. The powerful incinerator lobby had put many obstacles in the path of CPCB declaring pyrolysis as an approved technology for medical waste destruction. However, we finally won the battle with the issue of a Gazette notification in 2016 endorsing Plasma Pyrolysis for medical waste destruction.
Conclusions
Plasma pyrolysis technology is one of the many societally beneficial applications developed by FCIPT. One important lesson we learnt was that while it was relatively easy to master technology development, it was complicated to fight the battle with entrenched forces that resisted the introduction of advanced technologies, citing various reasons. Even government departments sometimes become tools of these retrograde forces.