



















ABSTRACT
Constipation is a common problem with multifactorial causes and different mechanisms. It can significantly impact quality of life as well as lead to other health problems. Symptoms can range from difficulty, straining or prolonged time in passing stool, infrequent bowel evacuations, change in stool consistency or a feeling of unsatisfactory evacuation. When constipation symptoms persist on most days and beyond 3 months, the problem is chronic and can often be associated with abdominal discomfort, bloating, cramps, appetite loss and overall decreased well-being. Though causes and risk or predisposing factors can often be identified, sometimes the constipation may be idiopathic. Since general physicians are the first point of contact for these symptoms, a careful and thorough history, general physical examination and appropriate investigations should be considered. Therapy with laxatives or new targeted drugs should be prescribed with monitoring of regularity, dosage, duration, clinical benefits and side effects.
Keywords: Constipation, Laxatives, Bowel, Stool, Bloating, Fiber
INTRODUCTION
Constipation is the difficulty in passing stool, which includes infrequent bowel evacuations, straining to pass stool, hard or lumpy stools, prolonged duration to evacuate or a feeling of not having evacuated fully or adequately. So, evidently constipation feels different for different people and its impact on everyday life can range from bothersome to very problematic. The month of December is observed globally as Constipation Awareness Month.
Everyone goes through episodes of constipation once in a while but when this is present for most days in the month, for at least 3 months or longer, the person is said to have chronic constipation. Most international definitions (like Rome criteria)1, label chronic constipation as <3 bowel evacuations in a week but this may be a drastic cut off for many populations (like India), where at least one bowel evacuation daily is commonly seen. Chronic constipation often leads to a feeling of abdominal discomfort, bloating, cramps, appetite loss and decreased well-being. Chronic idiopathic constipation (CIC) is a long-term form that has no identifiable organic cause. It is diagnosed based on symptoms like infrequent bowel movements, hard stools, straining and a feeling of incomplete evacuation.
RISK FACTORS
The risk of developing constipation increases with age (risk doubling >75 years) due to the weakening of muscles and decreased physical activity.2 Women are 3-4 times at higher risk of developing constipation. Constipation is more common in Asian and African ethnicities. Lifestyle factors such as type of diet (decreased fiber and increased processed items), low fluid and water intake, physical inactivity and sedentary lifestyle, improper bowel habits, psychological stress and intake of certain substances/medicines, all can lead to the development of constipation. Long-term illnesses and weakness or prolonged bed rest due to surgeries/illnesses also predispose to developing constipation.
TYPES OF CONSTIPATION
These are based on the probable cause and mechanisms of constipation (Table 1).3,4
Table 1: Types and Mechanisms of Constipation
| Type of Constipation | Cause | Main feature | Bowel movements | Transit Time |
| Functional (Normal Transit) | Low fiber and fluid intake.
Avoiding or delaying defecation* |
Reduced Stool Bulk
Difficulty in passing stool |
Normal | Normal |
| Slow Transit | Aging, bowel injury, nerve disorders, hormonal imbalance- pregnancy and certain drugs/medicines. | Reduced contracting ability of abdominal and bowel muscles.
Associated with bloating. |
Decreased | Increased |
| Dyssynergic | Injury to local muscles/nerves during childbirth, sexual abuse, aging, accidents and spinal cord injuries** | Incoordination of muscles of abdomen, pelvic floor and anal sphincter
Feeling of incomplete evacuation even after prolonged strain |
Normal/
decreased |
Normal |
| IBS-C# | Altered gut sensitivity to stretch/food, gut motility or transit time and gut fluid absorption-secretion. | Abdominal pain related to (relieved or brought on by) passing of stool, with change in form and frequency of stool | Variable | Variable |
| Mechanical Obstruction | Inflammation and scarring following injury, ulcers, infections, surgery, instrumentation, radiation, tumor/ cancerous growth, fecal impaction and rectoceles. | Local partial or complete obstruction (stenosis /stricture) prevents stools from passing out and present with almost sudden and complete constipation and a feeling of stools getting stuck | Reduced over time due to damage | Reduced due to block |
| Secondary | Diabetes, thyroid disorders, imbalances in calcium, magnesium or potassium, increased blood urea in liver disorders, neurological conditions like Parkinson’s, multiple sclerosis or stroke and heavy metal poisoning. | Presence of other clinical symptoms and lab findings | Affected | Reduced |
| *Suppression of the urge or avoiding passing stool: rushing to work/busy schedules, avoiding unpleasant / unhygienic toilets) or if there is a painful body condition making one avoid sitting for passing stools (hip/knee arthritis, injuries, recurrent boils, fissures in the anus, breathlessness on sitting/straining, etc.
**In those with nerve injuries and reduced sensations, the desire/urge to pass stool may not be appreciated consciously leading to enlargement (dilatation) of the large bowel/rectum and accumulation of stools (called megarectum/megacolon). #IBS can present as abdominal pain with constipation (IBS-C) or with diarrhea (IBS-D) or a mixed type (IBS-M) with alternate diarrhea and constipation. Sometimes gluten sensitivity can also be a cause. |
||||
MANAGEMENT
Constipation is not only a distressing condition affecting quality of life but can also increase the risk of conditions like hernia and piles (hemorrhoids). Therefore, it should be treated in a timely and effective manner.4,5 Certain investigations based on history, include blood and stool testing, referral for colonoscopy (if needed) and sometimes specific tests for gluten sensitivity or lactose intolerance may be advised.
- Diet and Lifestyle Modification
The general principles are to include more fiber like whole grains, vegetables and fruits and less processed and refined food. This is also the key to general good health, weight, sugar and fat management and keeping many lifestyle and metabolic conditions at bay.
- Fibers (Roughage)– These may be insoluble (add bulk to the stool) or soluble (absorb water, making the stools move smoothly). A balanced mix of insoluble fibers (whole grains, wheat bran, brown rice, prunes) and soluble fibers (oat bran, beans, lentils, peas and flaxseeds) should be incorporated in the diet. Vegetables and fruits are good sources of both insoluble and soluble fibers. While fibers provide additional health benefits like managing cholesterol, sugar and weight, some are fermented by gut bacteria that may temporarily aggravate flatulence, bloating or abdominal discomfort especially in IBS patients. Therefore, fiber intake should be kept to around 20-25 g/day in women and 30-35 g/day in men out of which 25-30% should come from soluble fibers.6 The fiber content of the food should be gradually raised. Some known constipating foods are meats, cheese, butter, fried foods, frozen foods, ice creams, processed grains and foods, high salt foods and sweetened sugary food items (cookies, cakes, pastries, etc).
- Water and Fluid intake – At least 1.5 to 2 litres/day is the recommended norm (this does not include beverages/other drinks). Alcoholic, sugary, aerated and carbonated drinks should be restricted as they increase the tendency to constipation.7 A morning warm/hot milk, coffee or tea works well to stimulate bowel movement but it is advisable to restrict them later in the day or evening as they are likely to constipate the next day. Fruit juices work well for people with a tendency to constipation.
- Lifestyle – A few habits go a long way to improve functional constipation. It’s prudent to ensure adequate time for passing stool by setting time for waking and not suppressing the urge to go to the toilet. Regular physical exercise (5 days/week), avoiding prolonged periods of sitting and some stretching/squatting exercises, helps to build abdominal muscle strength to aid in managing constipation. The brain and gut have an intricate connection, so stress or depression can lead to a slow down gut movement. Including de-stressing and relaxation techniques in daily routine can also contribute to smooth bowel functioning.
- Biofeedback – This involves the use of pressure measurements or averaged electromyographic activity within the anal canal to teach patients by using visual or auditory feedback, how to relax pelvic floor muscles, combined with more appropriate techniques for straining or increasing intra-abdominal pressure. In adults, randomized controlled trials show this form of biofeedback to be more effective than laxatives, general muscle relaxation exercises and drugs to relax skeletal muscles.8 Moreover, its effectiveness is specific to patients who have dyssynergic defecation and not slow transit constipation, making it a preferred treatment for dyssynergic defecation in adults. A therapy session may involve a manometric or EMG (electromyography) probe to measure muscle activity and a simulated balloon to help train the sensation of rectal filling. Biofeedback can be conducted in an office setting or with a home-based device. A typical protocol may involve 4-6 one-hour sessions, with reduced frequency over time as the patient improves.9 Periodic follow-up sessions at 6 weeks, 3 months and 6 months may provide additional long-term benefits.
2. Medicines
Laxative medicines are recommended in chronic and resistant constipation and are best used after medical consultation and investigations, which may include blood and stool testing. A colonoscopy may also be performed to rule out certain causes and sometimes specific tests for gluten sensitivity or lactose intolerance may be advised. Laxative medicines, even though available over the counter, need monitoring as irregular, inappropriate or too much use of laxatives can actually worsen the symptoms or condition in many people.10
Table 2: Medicine categories for Constipation
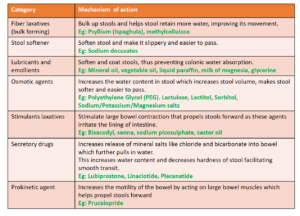
Magnesium salts include magnesium oxide, magnesium hydroxide (milk of magnesia), magnesium sulphate and magnesium citrate. Among these, magnesium oxide is least absorbed by the body, making it an effective osmotic laxative, with the unabsorbed magnesium increasing fluid pressure in the colon, stimulating bowel activity.11 Sodium sulfate (often combined with potassium and magnesium sulfate, as a saline laxative) increases the water content in the stool and stimulates gastrointestinal motility. It is used for general constipation and bowel cleansing before procedures like a colonoscopy. Sodium chloride (saltwater flush) involves drinking a mixture of salt and water to cause an urgent bowel movement due to the osmotic effect of the salt.
A combination of laxatives is also available (Ispaghula + Lactulose, PEG + Ispaghula, Milk of Magnesia + Liquid paraffin, etc). They are available as powders, liquids and capsules. They may also be used as an enema through the anus in a hospital setting for emptying the bowel before surgery/procedure or in acute severe constipation. Docusate sodium is a stool softener that makes the stool easier to pass by increasing the water and fat content of the stool.
Elobixibat is a prescription medication used to treat chronic constipation, particularly chronic idiopathic constipation (CIC) and this drug works by increasing the fluid and motility in the large intestine through a unique mechanism that affects bile acid circulation.12
Some of the side effects of laxative medicines include nausea, bloating, abdominal cramps, diarrhea and imbalance of mineral salts in the body.8 Palatability is also an issue that is often solved by flavouring the powder and liquid preparations. In the elderly, the leakage of stools (fecal incontinence) can be a disturbing side effect. Many of the over-the-counter preparations start to reduce in effectiveness over a period of time in chronic constipation cases and the need for larger and multiple doses may arise.
Newer drugs like linaclotide/plecanatide and prucalopride have shown effectiveness in chronic idiopathic constipation (CIC) not responding satisfactorily to conventional laxatives and also have the advantage of once-daily dosing.13
Vibrating capsules are a recent drug-free, FDA-approved treatment for chronic idiopathic constipation that work by mechanically stimulating the colon to increase motility.14 Swallowed at night, the capsule reaches the colon around 15 hours later, where it begins to vibrate in a programmed cycle to activate muscle contractions and promote bowel movements. Studies show the capsules are safe, effective and a viable option for those who don’t respond well to laxatives.
CONCLUSION
It is important for general practitioners to be well acquainted with the multifactorial mechanism and types of constipation and investigate thoroughly for all underlying causes and predisposing factors. Conventional therapies as well as new drugs should be used after evaluating patient risk-benefit and the type of constipation. Diet and lifestyle modification continue to be the cornerstone of therapy. Appropriate and timely specialty referral should be considered in resistant and unresponsive cases.
REFERENCES:
- Aziz I, Whitehead WE, Palsson OS, Törnblom H, Simrén M. An approach to the diagnosis and management of Rome IV functional disorders of chronic constipation. Expert Rev Gastroenterol Hepatol. 2020 Jan;14(1):39-46.
- Werth BL, Christopher SA. Potential risk factors for constipation in the community. World J Gastroenterol. 2021 Jun 7;27(21):2795-2817.
- Diaz S, Bittar K, Hashmi MF, et al. Constipation. [Updated 2023 Nov 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513291/
- Bharucha AE, Lacy BE. Mechanisms, Evaluation, and Management of Chronic Constipation. Gastroenterology, April 2020; 158(5):1232 – 1249.e3
- Hojo M, Shibuya T, Nagahara A. Management of Chronic Constipation: A Comprehensive Review. Intern Med. 2025 Jan 1;64(1):7-15.
- Akbar A, Shreenath AP. High Fiber Diet. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559033/
- Zhang, X., Liu, M., Wang, Y. et al.The impact of sugar-sweetened beverages consumption on constipation: evidence from NHANES. BMC Public Health 2025; 25;
- Chiarioni G, Heymen S, Whitehead WE. Biofeedback therapy for dyssynergic defecation. World J Gastroenterol. 2006 Nov 28;12(44):7069-74.
- Lee HJ, Jung KW, Myung SJ. Technique of Functional and Motility Test: How to Perform Biofeedback for Constipation and Fecal Incontinence. J Neurogastroenterol Motil 2013; 19(4): 532-537
- Bashir A, Sizar O. Laxatives. [Updated 2024 Jan 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537246/
- Mori H, Tack J, Suzuki H. Magnesium Oxide in Constipation. Nutrients. 2021 Jan 28;13(2):421.
- Agarwal, P., Jha, B.K., Somagoni, J. et al.Efficacy and safety of elobixibat in patients with chronic constipation—A randomized, multicenter, double-blind, placebo-controlled, parallel-group study from India. Indian J Gastroenterol 2025; 44: 336–344.
- Thayalasekeran S, Ali H, Tsai HH. Novel therapies for constipation. World J Gastroenterol. 2013 Dec 7;19(45):8247-51.
- Math PB, Ravi R, Hakami T, Das S, Patel N. Vibrating colon-stimulating capsule to treat chronic constipation: A systematic review. J Med Life. 2023 Jul;16(7):1050-1056.
1HOD, Gastroenterology & Hepatology, Kokilaben Dhirubai Ambani Hospital, Mumbai,
2Chief Editor, The Indian Practitioner and Medical Director, Dr Varsha’s Health Solutions, Mumbai.
