




















Abstract
Medical science has immense progress in drug discovery, diagnostics, technology and surgical techniques. However somewhere these advancements have come with a loss the human touch which has historically been the foundation of treatment. Patients have become data and hospitals are functioning more like corporates or businesses” that prioritise profits above all. Healing and recovery require open communication, transparency, clarity and empathy. Instead, if bottom lines, targets, inflated billing and commercial calculation become priority, patients are left confused, financially burdened, mentally stressed and disillusioned with the healthcare system. The soul of our healthcare system needs to be reclaimed and bridging of the wide chasm between corporate commercial interests and clinical patient care is the need of the hour.
Keywords: Corporate Hospitals; Healthcare; Health Insurance; Billing; Transparency; Communication and Patient Care.
Introduction
Technological progress cannot come or sustain at the cost of losing the human touch which is the basis of treatment. Patients cannot become cases or statistical data. While India’s medical technology has advanced, the moral infrastructure of the healthcare system has suffered a significant impact. The “temples and revered sanctuaries of healing” have, in many instances, been converted into “corporates and businesses” that prioritise profits above all, with doctors under pressure to meet targets rather than connect deeply with the patient’s needs and comfort. We are drifting from serving humanity and patients, to serving business interests and profit balance sheets.
On Doctor’s Day, we should reflect on what we practitioners have become today versus what we set out to be on choosing the medical profession. The Hippocratic Oath, solemnly taken by every doctor, clearly states: “I will use treatment to help the sick according to my ability and judgment, but never to injure or wrong them.”1 Yet, in today’s healthcare ecosystem, this sacred pledge is stands diluted with healing being less prioritised than billing and compassion being overridden by calculation. Patients are decreasingly being viewed as human beings in distress but more as revenue-generating units. Unnecessary diagnostic tests, lack of proper explanation of treatments initiated, drastically reduced interface of doctor-patient communication, prolonging of hospital stay, inflated bills, compromise of ethical care and in some cases even coercive treatment practices have become disturbingly common.2
Corporate-Private versus Government Healthcare Set-Up
Employment opportunities for doctors are now more attractive in the corporate sector rather than in government or doctor–owner facilities. Corporate employment is accompanied by widespread use of performance targets, an inflated cost of health care, increased compromise in practice ethics and a deterioration of doctor–patient relationships.3 Government set up frequently suffers from difficult working conditions, political and bureaucratic interference and poor pay.
In the light of the extreme competition that is faced by the fresh medical graduates who lack the client base and reputation of established practitioners, many doctors have no choice but to work for fixed salaries as understudies in bigger hospitals, while doctors working with corporate hospitals do not need to make investments or worry about the time required in setting up their own medical practice and renewal of medical licenses. Being in a well-known institution also has a positive effect on their patients as big hospitals with brands are assumed to employ the best doctors and they also provide more opportunities for greater professional advancement because of their better infrastructure. Corporate hospitals also offer higher security at the hospital premises to protect the doctors from the violence of patients.
Therefore, corporate private hospitals are increasingly emerging as the go-to or best option for practicing doctors.
Key Areas of Concern
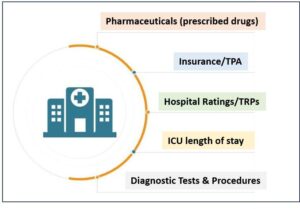
Figure 1 shows the main areas where there is absence of transparency and clear communication from the hospital to the patients. The nexus between hospitals, pharmaceuticals and insurance companies, is a well-known contributor to selection of medicines, decisions on investigations, procedures and surgery, duration of stay and inflated bills.4,5 Figure 1 showcase the sources of high revenue and commercial success of the healthcare facility, and key areas of absence of transparency and clear communication from the hospital to the patients. This often leaves patients with inflated bills, unanswered questions, confusion on what is essential and relevant and walking the tight rope between financial exploitation and what’s best for treatment, comfort and recovery, especially for the poor and middle class.6
Despite substantial increase in population eligible for state sponsored health insurance and rise in private health insurance companies, nearly 60% of families do not have a single person covered under any health insurance scheme. Further, the existing coverage is fragmented, with significant rural/urban and geographic variation within districts. Therefore, out of pocket expenses are very high with corporatisation of healthcare.7
The National Accreditation Board for Hospitals (NABH), is primarily a process and system auditor that sets benchmarks for healthcare facilities to improve patient safety, infection control and clinical outcomes. It provides voluntary and structured accreditation/certification programs for hospitals, clinics, labs and other healthcare organisations.8 Unfortunately, accreditation has become more procedural than principled, more bureaucratic than moral. There is a dire need of a coordinated effort by the Government, along with institutions such as the NABH, Central Consumer Protection Department (CCPD), Bureau of Indian Standards (BIS), National Medical Council (NMC) and the Indian Medical Association (IMA), to exercise effective moral, ethical and regulatory control over healthcare facilities.9
Figure 1: Key areas of hospital revenue and lack of transparent communication with patients
On-Ground Healthcare Scenario
As against the World Health Organization norm of one doctor per 1,000 people, India today has 1.8 doctors per 1000 people. However, India’s real doctor availability is 0.7 allopathic doctors per 1,000 population.10,11 The authenticity of this data has been questioned as many registered doctors do not practise. Some have died even though their names remain on the list of registered doctors. But there is no denying the fact that the number of doctors has increased principally due to the privatisation of medical education. About 10% of doctors are employed in government hospitals while a smaller percentage is attached to private hospitals. A substantial number of doctors are thus on their own and the key challenge is to get them attached to hospitals. Major cities boast high concentrations of medical professionals, while remote and rural regions continue to experience critical shortages. India also faces a dire shortage of nurses and midwives, lagging significantly behind the recommended density for supporting doctors effectively. In contrast, India has only 1.9 nurses and midwives per 1,000 people as against the WHO norm of 3-4 per 1,000 people.
With less than 1 bed per 1000 people, India’s hospital capability is lower than most developing Asian nations and also WHO’s recommended number of 3. India’s hospital bed per 1000 falls short of its own set standard of 2 beds per 1000 people.12 India accounts for 17% of the global population and 20% of the global disease burden, with 74% of its doctors residing in urban areas that serve 28% of the population.13 There are regional variations too. South and West India have 50% of doctors catering to 33% of the country’s population, while the remaining 67% have only 50% of doctors. Almost 65% of hospital beds are concentrated in just seven states — Karnataka, Kerala, Maharashtra, Tamil Nadu, Telangana, Uttar Pradesh and West Bengal. The number of doctors available varies too. While Delhi has roughly one doctor for 300 people, Jharkhand has one doctor for 8,000 people. Hence, though India may have exceeded the WHO norm, some states are facing an acute shortage of doctors, putting enormous pressure on the few government hospitals. Consequently, the quality of care is falling in these institutions.
Unattached doctors are also concentrated in urban areas. Those who are attached to private hospitals often work as consultants on a commission basis. Trained in private hospitals and often with a huge debt on their heads, some of these doctors face the pressure of earning handsomely, forcing them to indulge in commercial profit-making practices. This includes prescribing unnecessary, multiple and expensive medicines, diagnostic tests and even procedures. The government has now made it mandatory for doctors to prescribe generic names of medicines rather than brand names. This will give patients some freedom as they will be able to choose relatively less expensive brands. Nevertheless, they remain dependent on doctors when it comes to diagnostic tests and surgical procedures. No amount of regulation of private hospitals will do as the fundamental problem is of asymmetry in information and distribution.
Actionable points
India’s healthcare expenditure, roughly at 3% of its GDP, is among the lowest in the world and health expenditure as a percentage of GDP has been declining too.14 The only way to fix the shaky healthcare system is by increasing government expenditure on health.
Healthcare is not a commodity; it is a moral obligation and a constitutional responsibility. India urgently needs stringent laws, uncompromising enforcement and exemplary punishment for those who betray medical ethics or indulge in unfair practices.
To reclaim the soul of its healthcare system and bridge the widening gap between corporate interests and clinical care, a fundamental shift is needed in how healthcare is governed, centred on three imperatives:
- Legislative accountability requires the enactment of a national framework that holds hospitals legally and criminally liable for predatory billing and medically unjustified procedures.
- Transparent supervision must transform regulatory bodies from passive licensing offices into active guardians of ethics, while incorporating independent civil society oversight to curb the influence of medical lobbies.
- Decisive state action presupposes that the State can no longer remain a mute spectator to the unholy practices prevailing in the healthcare sector. We must dismantle systems that prioritise ledger entries over human lives.
Institutions such as the National Human Rights Commission (NHRC), State Human Rights Commissions (SHRCs) and allied bodies have, need to act decisively. Their silence in the face of injustice to patients amounts to nothing less than institutional abdication. The NHRC represents India’s commitment to ‘right to health’ and is closely monitoring this in terms health its accessibility, affordability and availability.15
Conclusion
It is time to reflect on what we practitioners have become today versus the ideals and ethics of the medical profession to which we were drawn. Healing, patient two-way communication, transparency, clarity in explanations and empathy need to be prioritised over bottom lines, targets, inflated billing and commercial calculation. Patients are human beings in distress who should be seen for their health condition and suffering and not as revenue- generating units. Unnecessary diagnostic tests, lack of proper explanation of treatments initiated, drastically reduced interface of doctor-patient communication, prolonging of hospital stay, inflated bills, compromise of ethical care and in some cases even coercive treatment practices need to be called out, curbed and controlled. The nation must reclaim the soul of its healthcare system. The time has come to bridge the widening chasm between corporatisation and commercial interests and clinical care and patient comfort, healing and recovery.
References
- The Hippocratic Oath. Congress.gov [online]. Available from https://www.congress.gov/117/meeting/house/114995/documents/HHRG-117-IF02-20220719-SD007.pdf
- The Fine Print [online]. India’s Healthcare Crisis: Profit Over Care and the Urgent Need for Reform. Jan 13, 2025. Available from https://nivarana.org/the-fine-print/indias-healthcare-crisis-profit-over-care-and-the-urgent-need-for-reform
- Javid Ahmad P, Samiran N. Has the corporatisation of our health sector in India helped us? Current Medicine Research and Practice. Jul–Aug 2022; 12(4):188-190.
- Kurpad SS. The pharmaceutical company–healthcare relationship: much ado about something. Indian Journal of Medical Ethics, [S.l.], April 2024; 9(2): 89.
- Ahuja S. Karmayog [online]. Bitter medicine: A nexus between hospitals and TPAs is leading to over-billing of the insured – a malady that the insurance regulator and insurance companies need to check promptly. Available from https://karmayog.org/personal-health/iebitter-medicine-a-nexus-between-hospitals-tpas-is-leading-to-over-billing-of-the-insuredfeb-16/
- Alexander GC, Casalino LP, Tseng CW, McFadden D, Meltzer DO. Barriers to patient-physician communication about out-of-pocket costs. J Gen Intern Med. 2004 Aug;19(8):856-60.
- Ambade M, Rajpal S, Kim R, Subramanian SV. Socioeconomic and geographic variation in coverage of health insurance across India. Front. Public Health. 2023;11:1160088.
- NABH Standards for Accreditation for Hospitals. 6th Edition, Jan 2025. Available from https://portal.nabh.co/images/Standards/NABH%20Hospital%20Accreditation%20Standard%206th%20Edition%20January%202025.pdf
- Ashwin BM. Deccan Herald [online]. BIS unveils standardized hospital billing to curb hidden cost, improve transparency. Dec 22, 2025. Available from https://www.deccanherald.com/india/karnataka/bengaluru/bis-unveils-standardised-hospital-billing-to-curb-hidden-costs-improve-transparency-3838928
- Health Policy UPSC [online]. WHO Clarifies Doctor Norm: India Below Global Health Workforce Benchmark. Nov 25, 2025. Available from https://www.understandupsc.com/who-clarifies-11000-doctor-norm-never-prescribed-india-far-below-global-health-workforce-benchmark/
- PIB [online]. Update on Medical Education in India. Dec 2, 2025. Available from https://www.pib.gov.in/PressReleasePage.aspx?PRID=2197614®=3&lang=1
- Jha S. South First [online]. India has only 0.79 beds per 1,000 population in government hospitals; Short by 2.4 million hospital beds. Dec 16, 2024. Available from https://thesouthfirst.com/health/india-has-only-0-79-beds-per-1000-population-in-government-hospitals-short-by-2-4-million-hospital-beds/
- Premanath, Manjunath. Beyond Numbers: Enhancing Healthcare Quality in India. APIK Journal of Internal Medicine. Oct-Dec 2025; 13(4):243-248.
- Panda HS, Rout HS, Jakovljevic M. Catastrophic health expenditure of inpatients in emerging economies: evidence from the Indian subcontinent. Health Res Policy Syst. 2024 Aug 12;22(1):104.
- Linga Murthy MS. Implementation of Right to Health in India: NHRC Role. International Journal of Creative Research Thoughts. Feb 2024; 12(2):96-103.