




















Abstract
India has a high prevalence of patients with hypertension and yet a large part of the population still remains undiagnosed. Newer guidelines recommending lower cut offs for the diagnosis, grading and therapeutic target of blood pressure are based on evidence of lower risk of cardiovascular disease, heart failure, stroke and dementia. However, in countries like India, this comes with a huge additional hypertensive population and patient inflow especially of young adults, increased healthcare expenditure and the risks of early initiation or intensification of anti-hypertensive therapy. It is important to develop diagnostic and treatment protocols based on the age, socioeconomic and cultural features and healthcare access of the Indian population to ensure optimal management of the country’s hypertension burden.
Keywords: Blood pressure cut off; Hypertension; AHA/ACC; Indian healthcare; PREVENT.
Introduction
The 2025-2026 American Heart Association and American College of Cardiology AHA/ACC introduced several major updates that reshape risk assessment, diagnosis and treatment strategy for hypertension.1 Replacing the 2017 guideline, the new document expands its scope, refines diagnostic criteria and adopts advanced risk estimation tools that align treatment decisions with overall cardiovascular risk. The guidelines prioritise a <130/80 mmHg target for most adults, with a target <120 mmHg when feasible, emphasising the new “PREVENT” risk calculator over the older Pooled Cohort Equations (PCE) model.
The new guidelines encourage the screening of young adults more actively due to elevated risks of heart and kidney disease later in life. The guideline points out that benefits for intensive lowering of BP not only include lower risk for heart disease, stroke and kidney disease, but also reduction in dementia risk. Specialised recommendations for older adults involve risk-based rather than age-based thresholds.1,2 World Hypertension Day is observed on May 17, 2026 and this reflects an opportunity to evaluate blood pressure diagnostic and target cutoffs risks and benefits, impact on the Indian healthcare systems and steps to be taken to ensure effective and appropriate management of the hypertension burden in India.
Core Guideline Updates
As compared to the older model PCE, PREVENT is a more advanced risk estimation tool for overall cardiovascular risk as it is independent of race and incorporates heart failure risk (apart from heart attack and stroke), kidney function (eGFR) and optional markers like glycated hemoglobin (HbA1C) and urine albumin/creatinine ratio (UACR). PREVENT covers a wider age range (30-79 vs. 40-79 years), provides both 10-year and 30-year risk estimates supporting long-term prevention and even incorporates provision for including a “Social Deprivation Index” based on zip code.3,4 Studies show PREVENT predictions better match actual observed risks in modern, diverse and treated populations, thereby improving predictive accuracy and supporting more individualised thresholds and treatment goals. PREVENT often results in lower risk scores, which could lead to fewer individuals being initiated on statin therapy compared to the 7.5% threshold often used with PCE.
The key updates include:
- Initiating medication for stage 1 hypertension (≥130/80 mmHg) based on a ≥7.5 risk on the new PREVENT calculator.
- Reliance on out-of-office and home blood pressure monitoring (HBPM) for accurate diagnosis and management.
- The target BP should be <130/80 mmHg, with strong encouragement for lower targets (<120 mmHg) to reduce stroke and dementia risk.
- Prioritising weight loss, sodium restriction, DASH (Dietary Approaches to Stop Hypertension)-style eating, physical activity, stress management and alcohol reduction.
- Potassium-based salt substitutes are now considered useful for most hypertensive patients (except in patients with chronic kidney disease or those on drugs that can cause hyperkalemia).
- Single-pill combinations recommended to improve adherence rather than starting with a single agent.
- Screening of all patients with resistant hypertension (or Stage 2) for primary aldosteronism, regardless of potassium levels.
| BP Category | Systolic BP | Diastolic BP | ||
| 1. | Normal | <120 mm Hg | and | <80 mm Hg |
| 2. | Elevated | 120 to 129 mm Hg | and | <80 mm Hg |
| 3. | Hypertension | |||
| Stage 1 | 130 to 139 mm Hg | or | 80 to 89 mm Hg | |
| Stage 2 | ≥140 mm Hg | or | ≥90 mm Hg | |
| · BP indicates blood pressure (based on an average of ≥2 careful readings obtained on ≥2 occasions.
· Adults with Systolic and Diastolic BP in 2 different categories should be designated to the higher BP category. · ESH-ESC guidelines 2024 considers BP categories as: 1. Non-elevated (BP<120/70); 2. Elevated (120–139/70–89 mmHg); 3. Hypertension (≥140/90 mmHg).5 · Indian Society of Hypertension (InSH) Consensus Guideline for the Management of Hypertension, 2025 recommends categorisation according to AHA-ACC 20256. |
||||
Table 1. Categories of Blood Pressure in Adults
Impact on India – Are We Prepared?
According to the National Health Mission, currently, hypertension awareness and control in India are poor, with only about 10–20% of cases in rural and urban areas being adequately controlled.7 Proponents suggest that lowering the blood pressure (BP) cutoff to <130/80 and 120/80 mmHg in India (from the old JNC8 pre-2017 guidelines cut off 140/90mm Hg) allows for earlier therapeutic lifestyle changes, which can curb the rising epidemic of cardiovascular diseases.8
However, this drastically increases the hypertension weighted prevalence from 18.5% to 45% and adjusted prevalence, from 29.7% to 63.8%, potentially labelling around 260 million additional adults (3 in every 5 adults) as hypertensive in India.9,10 The overall weighted/adjusted prevalence according to old and new guideline cutoffs among men is 21.2/39.4% and 52.3/69.9% respectively, while in women it is 18/29.3% and 41.5/48% respectively. The adjusted change in prevalence in different age categories is shown in Figure 1. The new threshold significantly impacts younger individuals, potentially causing the prevalence in people under 30 years to rise more than 4 times compared to doubling in elderly, leading to more of the youth being considered to have a chronic health condition.11
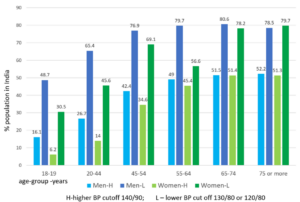
Figure 1 – Age Category Wise Adjusted Prevalence of Hypertension with Different Cot Offs.
In a US study, lower cut offs showed an additional 18.5% of adults ≥20 years to be eligible for initiation of pharmacological anti-hypertensive therapy, with another 10.8 % considered for medications if lifestyle modification prove insufficient.12 Increases in treatment eligibility were most pronounced among younger adults age 30–60 and those with obesity. Among adults currently being treated for hypertension an additional 17.6 % were considered eligible for treatment intensification if pursuing the preferred BP target of <120/80.
While the scenario above may be suitable for developed countries, for the developing world it is a huge rise in health expenditure. In a country like India where 72% population is less than 40 years of age, this new cut off can label every third youngster hypertensive. As sympathetic overdrive plays a major role in young population with hypertension, it may be inappropriate to have the same cut offs in young adults and elderly. Moreover, early use of anti-hypertensive drugs and aiming for lower targets, can be associated with side effects and light-headedness, fatigue and weakness. While promoting earlier intervention and reducing cardiovascular risks, this shift in cut off poses immense strain on India’s healthcare infrastructure and raises concerns regarding over-treatment, increased medication costs, potential side effects, as well as hypotension and acute kidney injury risk due to aggressive treatment, all leading to overall higher healthcare expenditure for both the government and individuals.11
With 70% of hypertension cases in India already undiagnosed, lower cutoffs may overburden healthcare especially the primary care system. Adopting a lower cutoff (e.g., 130/80 mmHg) could increase the prevalence of hypertension, creating a massive influx of new patients. The public health system, particularly Primary Health Centers (PHCs) and Health and Wellness Centers (HWCs), would face intensified demand for routine screenings, follow-up visits and long-term medication management. The increased diagnosis of hypertension would require a higher supply of anti-hypertensive drugs, potentially challenging existing supply chains in public health facilities and almost triple the economic burden on the healthcare system in India.
To manage the increased burden, Indian health infrastructure can utilise standard, simple and low-cost drug protocols at the primary care level to handle high patient volumes and train nurses and non-physician healthcare workers to manage hypertension and prescribe medication under protocol. Digital tools like the India Hypertension Control Initiative (IHCI) to track patients and developing other monitoring applications are important.13 Team-based management and culturally appropriate community-based group programs run by trained and supported ASHAs (Accredited Social Health Activists) are a successful and potentially scalable model for improving the control of hypertension in rural India.14
Conclusion
Lowering of the blood pressure cut off for hypertension has the upside of lower risk of heart disease, stroke and kidney disease, as well as possible reduction in dementia risk. However, this would require a rapid scaling-up of India’s primary health services, increased investment in medication supply chains and improved, decentralised care systems to manage a substantially larger patient population. Also the Indian healthcare fraternity would need to develop diagnosis and treatment protocols based on age, risk factors and socioeconomic conditions of various regions in India and ride the narrow road between the risks and benefits of lower BP targets, early introduction of antihypertensive medication and socio-economic impact of a higher proportion of the younger population being labelled as hypertensive and intensifying treatment in those already on lifestyle and/or minimal pharmacological interventions.
References:
- Jones DW, Ferdinand KC, Taler SJ, Johnson HM, Shimbo D, Abdalla M, et al. Peer Review Committee Members. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2025 Nov 4;86(18):1567-1679.
- Brown C, Clark D 3rd, Jones DW. Updates in the 2025 AHA/ACC Hypertension Guideline. Curr Hypertens Rep. 2026 Mar 17;28(1):19.
- Murphy BS, Hershey MS, Huang S, Nam Y, Post WS, McClelland RL, DeFilippis AP. PREVENT Risk Score vs the Pooled Cohort Equations in MESA. JACC Adv. 2025 Jun;4(6 Pt 1):101825.
- Zhou H, Zhang Y, Zhou MM, Choi SK, Reynolds K, Harrison TN, et al. Evaluation and Comparison of the PREVENT and Pooled Cohort Equations for 10-Year Atherosclerotic Cardiovascular Risk Prediction. J Am Heart Assoc. 2025 Feb 18;14(4):e039454.
- McEvoy JW, McCarthy CP, Bruno RM, Brouwers S, Canavan MD, Ceconi C, et al. ESC Scientific Document Group, 2024 ESC Guidelines for the management of elevated blood pressure and hypertension. European Heart Journal, 2024 Oct; 45(38): 3912–4018.
- Indian Society of Hypertension (InSH)Consensus Guideline for the Management of Hypertension, 2025. Available from https://9vom.in/journals/index.php/htnj/article/view/1097/909
- National Health Mission Hypertension Guidelines. Available from https://share.google/Nn3AtQwt8j3Db8Tyj. Cited May 2026.
- Mahdavi, M., Parsaeian, M., Mohajer, B, Modirian M, Ahmedi N, Yoosefi M. et al.Insight into blood pressure targets for universal coverage of hypertension services: the 2017 ACC/AHA versus JNC 8 hypertension guidelines. BMC Public Health 2020; 20:347.
- Gupta K, Jain V, Qamar A, Singal AK, Ramakrishnan S, Gupta R, Bajaj NS. Regional impact of updated guidelines on prevalence and distribution of blood pressure categories for hypertension in India: Results from the National Family Health Survey 4. Indian Heart J. 2021 Jul-Aug;73(4):481-486.
- Gupta K, Ramakrishnan S, Zachariah G, Rao JS, Mohanan PP, Venugopal K, et al; CSI-Great India BP Campaign Investigators. Impact of the 2017 ACC/AHA guidelines on the prevalence of hypertension among Indian adults: Results from a cross-sectional survey. Int J Cardiol Hypertens. 2020 Oct 7;7:100055.
- Maheshwari A, Verma N, Gupta A, Gupta VK, Patni B, Gupta B, et al. LOWERING CUTOFF FOR HYPERTENSION IS RAISING THREE TIMES HEALTH EXPENDITURE IN INDIA. Journal of Hypertension. April 2021. 39():p e272.
- Sayed A, Peterson ED, Navar AM. Implications of the 2025 AHA/ACC high blood pressure guidelines on the initiation and intensification of blood pressure-lowering medications among US adults. Am J Prev Cardiol. 2026 Jan 18;25:101400.
- Kaur P, Kriina M, Ganeshkumar P, Kunwar A, Sharma M, Shivashankar R. India Hypertension Control Initiative Collaboration; Bhargava B. Scaling India Hypertension Control Initiative strategies to 15 states-treatment outcomes and risk factors for uncontrolled blood pressure, India: a cohort study, 2018-2021. BMJ Open. 2025 Nov 28;15(11):e106372.
- Riddell MA, Mini GK, Joshi R, Thrift AG, Guggilla RK, Evans RG, et al. ASHA-Led Community-Based Groups to Support Control of Hypertension in Rural India Are Feasible and Potentially Scalable. Front Med (Lausanne). 2021 Nov 22;8:771822.

