



















Abstract
GLP1-RA semaglutide and tirzepatide are becoming commonly prescribed medicines for weight loss. With their fast-paced increase in market share, this is an apt time to review their medical evidence and data from comparative studies to evaluate their efficacy and safety. It is important to understand both benefits and caution with these drugs, so that patients may be given guidance on reporting side effects, be alerted for warning and red-flag signs and appropriately monitored by the prescribing clinician for adverse drug reactions, in order to derive best clinical outcomes.
Keywords: GLP1-RA, Weight loss, Semaglutide, Tirzepatide, High BMI, Obesity
Introduction
Glucagon-like peptide-1 receptor agonist (GLP1-RA) are drugs which are used for both type 2 diabetes and weight management, mimicking the body’s natural GLP1 hormone. Their mechanism of action involves enhancing glucose-dependent insulin secretion from the pancreas, slowing gastric emptying and reducing glucagon release.1 Activation of GLP1 receptors in the hypothalamus helps decrease appetite, increase satiety and reduce food cravings, leading to weight loss. Here we review GLP1-RAs in weight loss for non-diabetics. While semaglutide and liraglutide are GLP1RAs in this space, tirzepatide is an analog of the hormone glucose-dependent insulinotropic polypeptide (GIP) and helps stimulate insulin release in response to high blood sugar, in addition to activating the GLP-1 receptor. This dual action leads to improved glycemic control, increased feeling of fullness and reduced appetite.2 GLP1-RA can also help lower the risk of major adverse cardiovascular events (MACE – heart attack, stroke or cardiovascular-related death), lower the risk of chronic kidney disease (CKD) worsening or kidney failure and also cause some weight loss.3
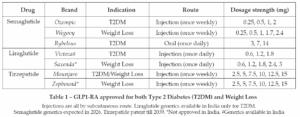
Interestingly, for the same drug molecule, different brands have been launched globally for weight management and type 2 diabetes (Table 1). For weight loss, the approved GLP1-RAs are indicated for adults who have obesity (body mass index [BMI] of 30 kg/m² or greater) or are overweight (BMI of 27 kg/m² or greater) with at least one weight-related health condition like high blood pressure, type 2 diabetes, high cholesterol or obstructive sleep apnea. These drugs can help lose 5-10% of body weight or more, over a year.4 Wegovy and Saxenda are also indicated for adolescents (aged 12 and older) who have obesity, weigh more than 60 kg and have an initial BMI corresponding to 30 kg/m². While Semaglutide (Wegovy) is approved in India, Saxenda and Zepbound are not. Tirzepatide (Mounjaro) is approved in India for weight loss also. Liraglutide is only approved for T2DM, not weight loss, in India.
Therefore, among GLP1-RA for weight loss in India, we have mainly 2 approved branded drugs: Semaglutide (Wegovy) and Tirzepatide (Mounjaro) injections.
Making Evidence Based Prescribing Decisions
While the patient indication in terms of weight and BMI remains the same, it is important to know factors that can affect prescribing decisions. Pricing for both is not widely different to be a deciding factor especially in patients going in for weight management. In terms of head-to-head comparison of efficacy two recent studies in 2024-25 are discussed below.
Efficacy
SURMOUNT trials (1-4) evaluated the efficacy and safety of Tirzepatide in overweight obese with and without T2DM, as well as for long-term maintenance. SURMOUNT-5 was a comparative phase 3b study with 750 adult participants with obesity without type 2 diabetes randomly assigned in a 1:1 ratio to receive the maximum tolerated dose of tirzepatide (10 mg or 15 mg) or the maximum tolerated dose of semaglutide (1.7 mg or 2.4 mg) subcutaneously once weekly for 72 weeks.5 Weight loss in the 2 groups (by least-squares mean % change in weight at week 72) was −20.2% with tirzepatide and −13.7% with semaglutide (P<0.001;95% CI). The least-squares mean change in waist circumference was −18.4 cm with tirzepatide and −13.0 cm with semaglutide (P<0.001;95% CI). Participants in the tirzepatide group were more likely than those in the semaglutide group to have weight reductions of at least 10%, 15%, 20% and 25%.
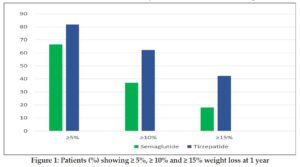
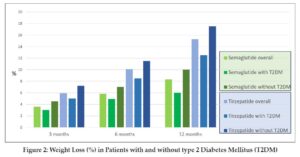
In a propensity score–matched population, among 41,222 adults meeting the study criteria, patients receiving tirzepatide were significantly more likely to achieve weight loss ≥5% (HR 1.76, 95% CI), ≥10% (HR 2.54) and ≥15% (HR 3.24) than semaglutide.6 The % patients showing ≥5%, ≥10% and ≥15% weight loss at 1 year is shown in Figure 1. This study included both overweight and obese, as well as those with T2DM and without. Weight loss was more prominent in those without T2DM in both groups as seen in Figure 2 but in all cases, was higher for tirzepatide.
A metanalysis of the two randomized controlled trials (RCTs) and five retrospective cohorts showed that compared with the semaglutide, tirzepatide could produce significantly greater weight loss (mean difference MD = 4.23; 95% CI; P < 0.01).7 The better results with tirzepatide were maintained in both RCTs and retrospective cohorts. The pooled analysis provides evidence that tirzepatide is better than semaglutide in reducing body weight, regardless of study design. A dose-response relationship exists and the weight loss magnitude increases with the dose or duration of tirzepatide. Another metanalysis compared the most closely matched trials conducted with semaglutide 2.4 mg and tirzepatide – one trial each of semaglutide 2.4 mg (STEP-1) and tirzepatide 5, 10 and 15 mg (SURMOUNT-1) in obese or overweight people without T2D and one trial each of semaglutide 2.4 mg (STEP-2) and tirzepatide 10 and 15 mg (SURMOUNT-2) in overweight people with T2D.8 It was found that tirzepatide 10 and 15 mg produced 4-5.4 % additional weight loss, 0.4% additional HbA1c reduction, than with semaglutide 2.4 mg. Another metanalysis reported a weight loss of 5.27 and 9.57 kg with tirzepatide 5 and 15 mg, respectively and 2.52 and 4.97 kg with semaglutide 0.5 and 2.0 mg, respectively, through a metanalysis of two head-to-head comparison RCTs of tirzepatide and semaglutide.9
Safety
- Gastrointestinal and Renal
The most common adverse events in both treatment groups in SURMOUNT-5 were gastrointestinal (GI) and most were mild to moderate in severity and occurred primarily during dose escalation, however treatment discontinuation due to GI side effects were lower in tirzepatide group (6% vs 8%).5 In other studies, too rates of gastrointestinal AEs were similar between group. The metanalysis showed that tirzepatide 10 and 15 mg produced fewer gastrointestinal side effects, than semaglutide 2.4 mg. An analysis of 13 RCTs that investigated the effects of semaglutide and tirzepatide on GI, hepatic, pancreatic and biliary outcomes in a total, 26,894 participants with obesity but without diabetes were revealed 30.81% of participants receiving semaglutide experienced GI issues, while only 12.7% in the control group did. For tirzepatide, 79.8% of participants experienced GI events, a figure notably higher than the 25% observed in the control group.10 Overall GI adverse events were 1.8-2.9 times higher with both agents (higher for tirzepatide than semaglutide).
Semaglutide increased gallbladder-related disorders like acute cholecystitis and particularly cholelithiasis, by over 2.6 times, while tirzepatide showed no significant biliary risk. Neither agent significantly increased hepatic or pancreatic adverse events. However, while prescribing these GLP1-RAs, monitoring of GI side effects is important especially in people with history of acid reflux, dyspepsia and constipation and its use avoided in patients with severe gastroparesis and a history of pancreatitis or gallbladder disease.
Recently, a pooled analysis of 7 retrospective cohort studies involving > 5 million patients revealed a significantly increased (more than two-fold) risk of colorectal cancer among patients receiving GLP-1 RAs (RR, 2.31; 95% CI, 1.82–2.93; heterogenicity = 36%; p < 0.0001). These findings highlight the need for further long-term, large-scale clinical trials to elucidate the relationship between GLP-1 RAs and cancer risk. Clinicians should consider these results when prescribing GLP-1 RAs, particularly in patients with risk factors for colorectal cancer.11
In a large study of more than 20,000 patients, semaglutide versus tirzepatide showed an increased risk of acute kidney injury (AKI – OR 1.96, CI 1.56 – 2.45, P < 0.0001), underscoring the importance of monitoring kidney function in patients on semaglutide.12
- Ophthalmic
While ophthalmic side effects of non-arteritic anterior ischemic optic neuropathy (NAION) have been seen in patients on semaglutide treatment for both overweight/obesity and T2DM (though risk is higher in T2DM which is an independent risk factor for ON), considering the extensive number of participants involved in randomized clinical trials and the large global population using GLP-1RAs, any absolute risk of developing NAION due to semaglutide use is likely to be very low and not confirmed, showing the need for additional data-driven research to verify or disprove such a link.13 A propensity score matching in 159 398 T2DM patients with a 2-year follow-up, showed 0.04% with NAION in the semaglutide or tirzepatide group and 0.02% with NAION in the matched comparison group (HR 1.76 ; 95% CI).14 No association was found with other disorders of the optic nerve or visual pathways. But advise to report any visual disturbance immediately should be given to all patients.
- Psychiatric
Recent data indicate that as GLP1-RAs semaglutide and tirzepatide affect appetite regulation, mood and reward pathways, they can improve sleep and reduce compulsive eating and addictive behaviour but also have potential to cause depression, anxiety, altered emotional processing and rarely suicidal ideation and such cases have been reported, although causality remains under investigation. Therefore, vigilance is needed to detect and manage such adverse events and more studies needed to clarify mechanisms and patient-specific risk factors.15
- Contraindications
Both semaglutide and tiraepatite have a boxed warning and contraindication for people with personal or family history of medullary thyroid carcinoma (MTC) and patients with multiple endocrine neoplasia syndrome type 2 (MEN 2), a genetic condition that causes tumours in endocrine glands, as animal studies showed a risk of thyroid C-cell tumours and it is unknown if this same risk applies to humans.16 Other contraindications include hypersensitivity or previous reaction to a GLP-1 RA and are not recommended for pregnant or breastfeeding women, as safety in these populations has not been established. The effectiveness of oral hormonal contraceptives, can be reduced, so a non-oral or barrier method is recommended for four weeks after starting and after any dose increase of these two drugs.
Conclusion
Considering absolute efficacy and amount of weight loss, tirzepatide appears to have an edge. Safety concerns seem similar and there is more long-term adverse event data analysis available for semaglutide as compared to tirzepatide. As compared to a pharmaceutical or regulatory perspective, a clinician’s outlook requires a holistic risk-benefit assessment comprising of all the risks inherent in the molecule, the comorbidities, versus the actual clinical benefit. Other options in conjunction with lifestyle modification should also be explored by the clinician making GLP1-RA optional and not indispensable.
Currently as both are branded drugs, cost and access may not be deciding factors. However, once semaglutide goes off-patent in 2026, far cheaper generics may flood the market, when cost may become a factor to consider especially when prescribing to low-mid socioeconomic strata or/and when the amount of weight loss needed may be moderate to achieve BMI and clinical goals. While prescribing these GLP1-RA, monitoring of side effects is important. More real-world data with tirzepatide use for weight loss will add insights. There are also new drugs for weight loss on the horizon to keep a watch for.
References
- Collins L, Costello RA. Glucagon-Like Peptide-1 Receptor Agonists. [Updated 2024 Feb 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551568/
- Zheng, Z., Zong, Y., Ma, Y. et al.Glucagon-like peptide-1 receptor: mechanisms and advances in therapy. Sig Transduct Target Ther 2024; 9, 234.
- Badve SV, Bilal A, Lee MMY, Sattar N, Gerstein HC, Ruff CT, McMurray JJV, Rossing P, Bakris G, Mahaffey KW, Mann JFE, Colhoun HM, Tuttle KR, Pratley RE, Perkovic V. Effects of GLP-1 receptor agonists on kidney and cardiovascular disease outcomes: a meta-analysis of randomised controlled trials. Lancet Diabetes Endocrinol. 2025 Jan;13(1):15-28.
- Jensterle M, Rizzo M, Haluzík M, Janež A. Efficacy of GLP-1 RA Approved for Weight Management in Patients With or Without Diabetes: A Narrative Review. Adv Ther. 2022 Jun;39(6):2452-2467.
- Aronne LJ, Horn DB, le Roux CW, Ho W, Falcon BL, Gomez Valderas E, et al. SURMOUNT-5 Trial Investigators. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity. N Engl J Med. 2025 Jul 3;393(1):26-36
- Rodriguez PJ, Goodwin Cartwright BM, Gratzl S, et al. Semaglutide vs Tirzepatide for Weight Loss in Adults with Overweight or Obesity. JAMA Intern Med.2024;184(9):1056–1064.
- Aamir AB, Latif R, Alqoofi JF, Almarzoq FA, Fallatah JO, Hassan GA, Saab FAAAA. Comparative Efficacy of Tirzepatide vs. Semaglutide in Reducing Body Weight in Humans: A Systematic Review and Meta-Analysis of Clinical Trials and Real-World Data. J Clin Med Res. 2025 May;17(5):285-296.
- Singh A, Singh AK, Singh R, Misra A. Comparative efficacy and safety of semaglutide 2.4 mg and tirzepatide 5-15 mg in obesity with or without type 2 diabetes: A systematic review of Phase 3 clinical trials. Diabetes Metab Syndr. 2025 Mar;19(3):103212.
- Karagiannis T, Malandris K, Avgerinos I, Stamati A, Kakotrichi P, Liakos A, Vasilakou D. et al. Subcutaneously administered tirzepatide vs semaglutide for adults with type 2 diabetes: a systematic review and network meta-analysis of randomised controlled trials. Diabetologia. 2024;67(7):1206–1222.
- Safwan M, Bourgleh MS, Alotaibi SA, Alotaibi E, Al-Ruqi A, El Raeya F. Gastrointestinal safety of semaglutide and tirzepatide vs. placebo in obese individuals without diabetes: a systematic review and metanalysis. Ann Saudi Med. 2025 Mar-Apr;45(2):129-143.
- Zhong Y, Wu T, Khan NU. Association between GLP-1 receptor agonists as a class and colorectal cancer risk: a meta-analysis of retrospective cohort studies. BMC Gastroenterol. 2025 Aug 22;25(1):614.
- Shwani Z. Battle of the Weight-Loss Titans: Semaglutide vs Tirzepatide – Which is Safer? The American Journal of Gastroenterology Oct 2024;119(10S):p S1501.
- Narayanan, V, Purohit N. The Risk of Non-Arteritic Anterior Ischemic Optic Neuropathy (NAION) and Worsening Diabetic Retinopathy (DR) With Semaglutide. Asian Journal of Research and Reports in Ophthalmology 2025; 8 (1):94-100.
- Wang L, Volkow ND, Kaelber DC, Xu R. Semaglutide or Tirzepatide and Optic Nerve and Visual Pathway Disorders in Type 2 Diabetes. JAMA Netw Open. 2025 Aug 1;8(8):e2526327.
- Santos RI dos, de Lima Gambarra NC, Magalhães AWD, Guimarães PHS. Psychiatric Effects Associated with GLP-1 and GIP Agonists: A review of Semaglutide and Titzepatide. Asclepius International Journal of Scientific Health Science, São José dos Pinhais, Paraná, 2025;4(7):509–518.
- Shilyansky JS, Chan CJ, Xiao S, Gribovskaja-Rupp I, Quelle DE, Howe JR, et al. GLP-1R agonist promotes proliferation of neuroendocrine neoplasm cells expressing GLP-1 receptors. Surgery. 2025 Mar;179:108943.
1Medical Affairs Consultant and Family Physician, Holistic Evidence-based Advice, Research and Treatment (H.E.A.R.T), Mumbai
2Chief Editor, The Indian Practitioner and Medical Director, Dr Varsha’s Health Solutions, Mumbai.
