



















Abstract
Vitamin D is available in various dosage forms and strengths for supplementation and also as combinations with calcium and other components, for bone health and reduction of osteoporosis risk. In addition, calcitriol, its active form is also available for supplementation individually and in combinations. There are also vitamin D or calcitriol analogs that are available globally and being introduced into the bone health and osteoporosis therapy space in India. Here is presented the overview of the regulation of calcium and the action of vitamin D and other important hormones, vitamins and minerals in bone formation and health. The positioning, indication and clinical usage of vitamin D, calcitriol and its analogs for bone health is thereby outlined.
Keywords: Vitamin D, Calcidiol, Calcitriol, Vitamin D analogs, Calcium, Bone health, Osteoporosis
Introduction
Vitamin D (D3) is synthesized in our body from cholesterol in the presence of sunlight. This synthesized Vitamin D3 as well as dietary vitamin D3 (from animal foods) and D2 (from plant foods) is activated in a 2-step process, first in the liver to its 25-hydroxy form (calcidiol – 25(OH)D) which is measured in blood and then in the kidney to its 1,25-dihydroxy form (calcitriol). Therefore, calcitriol is the active form of vitamin D mediating all its physiological effects.
Supplements containing various doses of vitamin D as well as combinations with calcium have flooded the market. In addition, many of these combinations also contain calcitriol instead of vitamin D, along with other components. We should understand the physiological role and clinical relevance of each component before making prescribing decisions in the space of bone health and preventing osteoporosis (20th October is observed as World Osteoporosis Awareness Day annually).
Hormonal Regulation of Calcium
Calcitriol and Parathyroid hormone (PTH)
Calcitriol’s primary functions include regulating calcium and phosphorus levels, which is essential for bone mineralization. It increases calcium and phosphorus absorption from the intestines, promotes calcium reabsorption in the kidneys and stimulates bone mineralization by calcium and phosphorus uptake by bones. Calcitriol is also known to have neuroprotective effects and is involved in immune function and regulation.
PTH stimulates the enzyme 1 alpha-hydroxylase responsible for the final step of conversion to calcitriol in the kidney while this enzyme undergoes feedback suppression by high levels of its own product, calcitriol. Calcitriol production can be low or absent in certain conditions, most notably chronic kidney disease (CKD) and low PTH due to hypoparathyroidism. Other conditions include increased blood phosphorus levels stimulating fibroblast growth factor (FGF-23) production, which inhibits calcitriol synthesis and rare genetic conditions that interfere with vitamin D metabolism and calcitriol production.
Calcitriol and PTH both increase calcium absorption from the gut and calcium reabsorption from the kidney tubules. However, their effects are opposing on the bone, where calcitriol promotes uptake of calcium and bone synthesis, while PTH promotes bone breakdown and release of calcium into the blood.1
Calcitonin
It is a hormone produced by the thyroid gland that lowers blood calcium levels by reducing the breakdown of bone and increasing calcium excretion by the kidneys. It acts to oppose PTH which raises blood calcium levels.2
Estrogen
It protects bones by decreasing the activity of osteoclasts and increasing the activity of osteoblasts thereby preventing bone loss and maintaining bone mineral density (BMD). Fall in this hormone post-menopause leads to increased bone resorption, reduced bone mass and increased risk of osteoporosis.3
Role of Other Minerals and Vitamins
Magnesium
Magnesium promotes healthy bone density by aiding calcium absorption, regulating PTH and supporting bone-forming osteoblast activity while inhibiting bone-resorbing osteoclasts. Magnesium increases calcium absorption in the gut and also stimulates 1 alpha-hydroxylase in the kidney to form calcitriol. Magnesium can stimulate the release of calcitonin and help pull calcium from the blood into the bones, maintaining adequate levels for bone density.
Magnesium acts on the same calcium-sensing receptors (CaR) on the parathyroid glands that detect high calcium levels. High magnesium through these receptors inhibits PTH secretion. However, magnesium is essential for the function of G-proteins that couple to the CaR, thereby low magnesium can hinder the signalling pathway necessary for normal PTH release. Therefore, optimum amounts of magnesium regulate PTH and calcium levels appropriately. In chronic haemodialysis, high dialysate magnesium can lead to lower serum PTH levels (secondary hypoparathyroidism). Adequate magnesium intake is linked to higher bone mineral density and reduced risk of osteoporosis and fractures.
An adequate calcium to magnesium ratio (Ca:Mg) in the diet is ideally around 2:1, generally within the range of 1.7:1 to 2.6:1, by weight. A ratio more than that can interfere with magnesium absorption. Therefore, increasing calcium intake, especially through supplements, without sufficient magnesium may have negative implications on bone and general health.4
K2-7
It is a form of vitamin K, that plays a vital role in bone health by activating osteocalcin, a protein that binds calcium to bone, thereby facilitating bone mineralization and inhibiting osteoclast activity to reduce bone loss. Given with calcium, K27 can help divert calcium to bone and reduce vascular deposition and plaque formation by activating the matrix Gla protein (MGP), which inhibits calcium from depositing in arteries.5
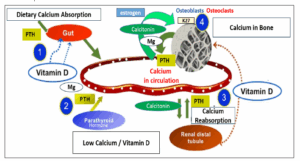
Figure 1: Regulation of Calcium in Blood and Bone6-8
Vitamin D supplementation
Vitamin D has a recommended daily allowance of 400 International Units (IU) in infants and 600 IU in children and adults in accordance with ICMR 2020-21.9 It is available in combination with calcium for daily supplementation as well as individually as shots (weekly doses 60,000 IU and injections up to 6 lakh IU). To maintain adequate blood levels, the Endocrine Society recommends an intake of daily Vitamin D of 400 to 1000 IU for adults and children and 1000-2000 IU for pregnant-lactating women and for osteoporosis prevention.10 These doses of Vitamin D are usually available in combination with calcium for routine supplementation. However, variations in recommendations are based on risk factors, sun-exposure, dietary factors, race, comorbidities and individual symptoms. Generally, it takes a few weeks (up to 12 weeks) of taking daily vitamin D supplements for vitamin D levels in the body to rise (100 IU Vitamin D daily is expected to raise blood levels of 25(OH)D by 1 ng/ml after a few weeks).
Injections and weekly high doses as shots/sachets are recommended when there is documented vitamin D insufficiency.11 Vitamin D levels are typically measured in the blood as 25-hydroxyvitamin D (calcidiol – 25(OH)D) – Deficient:<20 ng/mL; Insufficient: 20-30 ng/mL; Sufficient: >30 ng/mL. The Endocrine Society recommends a preferred range of 40 to 60 ng/mL. If in low sufficient or insufficient range, then 60,000 IU of Vitamin D once a week for 8 weeks is recommended to achieve a serum 25OHD above 30 ng/mL, followed by maintenance therapy of 1500–2000 IU/day or 60,000 IU monthly.12 Deficient cases may be given a single injection of up to 6L IU followed by oral maintenance as described and monitoring of blood Vitamin D levels.13
Supplementation of Calcitriol
Calcitriol systemic supplementation is FDA-indicated to control renal dialysis associated hypocalcemia, secondary hyperparathyroidism in patients with chronic kidney disease and patients with hypoparathyroidism and pseudohypoparathyroidism (a rare genetic disorder where the body doesn’t respond PTH leading to hypocalcemia and hyperphosphatemia despite normal or elevated levels of the PTH itself).
Therefore, the main rationale of giving calcitriol is when impaired kidney function or lack of PTH action prevents the activation by the body of vitamin D to calcitriol, its active form.
Calcitriol may be administered intravenously 1 ug/ml solution as a bolus dose given at the end of a hemodialysis session or orally (0.25, 0.5 ug capsules).14 When giving the activated form of vitamin D directly, the risk of hypercalcemia and hypercalciuria (causing kidney/ureteric stones) should be kept in mind. Therefore, calcitriol is started at 0.25 ug/d, increased by 0.25 ug/d at 4 to 8 weeks to reach a dose of 1 ug/d or 0.5 ug/bid (maximum 2 ug/d). During this titration period, serum calcium levels are monitored twice weekly during titration and monthly once the optimal dose is reached. That is why in fixed dose combinations, calcitriol is kept in its basic dose of 0.25 ug once daily.
Osteoporosis risk: Calcitriol in a low basal dose of 0.25 ug/d combined with calcium and K27, is sometimes used as a bone-health supplement instead of calcium-vitamin D, to reduce osteoporosis risk in elderly men and post-menopausal women with high osteoporosis risk factors and comorbidities, leading to possible age-related or comorbidity-induced decline in hepatic and renal function, that may lower conversion of vitamin D to its active form.15 The risk of hypercalcemia and hypercalciuria with such a low basal dose of calcitriol is considered minimal.
Calcitriol analogs for bone health
These include alfacalcidol and eldecalcitol. Eldecalcitol is similar to calcitriol – specifically a 2β-hydroxypropyloxy derivative of 1α,25-dihydroxyvitamin D3 (calcitriol). Eldecalcitol also has independent (of vit D receptor) activity on bone resorption that sets it apart from calcitriol as not just the activated form of vitamin D.16 Alfacalcidol (1α-hydroxycholecalciferol) is a prodrug like vitamin D and needs one step hepatic activation to calcitriol.17
For Eldecalcitol, the phase II/III study in Japan found the 0.75 ug/d and 1 ug/d dose improved hip bone mineral density (BMD) and reduced bone turnover markers (BTMs) in addition to improved vertebral BMD. Transient hypercalcemia was least with 0.75 dose (5% compared to 7% and 23% in 0.5 and 1 ug group).16,18 Therefore, it was concluded that 0.75ug is the ideal dose for both lumbar and hip BMD improvement with least risk of hypercalcemia. Similar results have been seen with alfacalcidol 1 ug/d, however, comparative studies show eldecalcitol can effectively inhibit bone resorption strongly, with a similar effect on bone formation and a comparable effect on urinary Ca excretion and was superior for improving vertebral fracture risk and BMD than alfacalcidol, suggesting that eldecalcitol may have a better osteoprotective effect than alfacalcidol.19,20
Conclusion
Vitamin D and calcitriol, as well as analogs are available for bone health and reduction of osteoporosis risk. It is important to understand the regulation of calcium and the action of vitamin D and other important hormones, vitamins and minerals in bone formation and health. Thereafter, the positioning, indication and clinical usage of vitamin D, calcitriol and its analogs for bone health and osteoporosis can be well defined with clinical relevance and applied effectively for appropriate prescribing practices. Treatment with analogs for both prevention and treatment of osteoporosis is still at its nascent stage in India and the future launch and availability of these products in India will further enhance the clinical armamentarium of osteoporosis prevention and management in our country.
References
- Khan M, Jose A, Sharma S. Physiology, Parathyroid Hormone. [Updated 2022 Oct 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499940/
- McLaughlin MB, Awosika AO, Jialal I. Calcitonin. [Updated 2023 Aug 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537269/
- Cauley JA. Estrogen and bone health in men and women. Steroids. 2015 Jul;99(Pt A):11-5.
- Rondanelli M, Faliva MA, Tartara A, Gasparri C, Perna S, Infantino V, et al. An update on magnesium and bone health. Biometals. 2021 Aug;34(4):715-736.
- Jadhav N, Ajgaonkar S, Saha P, Gurav P, Pandey A, Basudkar Vet al. Molecular Pathways and Roles for Vitamin K2-7 as a Health-Beneficial Nutraceutical: Challenges and Opportunities. Front Pharmacol. 2022 Jun 14;13:896920.
- Holick, Michael F. Vitamin D: the underappreciated D-lightful hormone that is important for skeletal and cellular health. Current Opinion in Endocrinology & Diabetes Feb 2022; 9(1):87-98.
- Lips P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev. 2001 Aug;22(4):477-501.
- DeLuca HF. Overview of general physiologic features and functions of vitamin D. Am J Clin Nutr 2004;80(suppl):1689S–96S.
- FSSAI 2020-2021. RDA. Available from https://www.fssai.gov.in/upload/advisories/2021/07/60f1798019f94Direction_RDA_16_07_2021.pdf
- Chauhan K, Shahrokhi M, Huecker MR. Vitamin D. [Updated 2023 Apr 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441912/
- Bleizgys A. Vitamin D Dosing: Basic Principles and a Brief Algorithm (2021 Update). Nutrients. 2021 Dec 10;13(12):4415.
- Gupta N, Farooqui KJ, Batra CM, Marwaha RK, Mithal A. Effect of oral versus intramuscular Vitamin D replacement in apparently healthy adults with Vitamin D deficiency. Indian J Endocrinol Metab. 2017 Jan-Feb;21(1):131-136.
- Diamond TH, Ho KW, Rohl PG, Meerkin M. Annual intramuscular injection of a megadose of cholecalciferol for treatment of vitamin D deficiency: efficacy and safety data. Med J Aust. 2005 Jul 4;183(1):10-2.
- Lung BE, Komatsu DEE. Calcitriol. [Updated 2025 Mar 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526025/
- Peppone LJ, Hebl S, Purnell JQ, Reid ME, Rosier RN, Mustian KM, Palesh OG, Huston AJ, Ling MN, Morrow GR. The efficacy of calcitriol therapy in the management of bone loss and fractures: a qualitative review. Osteoporos Int. 2010 Jul;21(7):1133-49.
- Noguchi Y, Kawate H, Nomura M, Takayanagi R. Eldecalcitol for the treatment of osteoporosis. Clin Interv Aging. 2013;8:1313-21.
- Jewell R, Alfacalcidol, xPharm: The Comprehensive Pharmacology Reference, Elsevier, 2007:1-5. Available from https://www.sciencedirect.com/science/article/abs/pii/B9780080552323611845
- Liu H, Wang G, Wu T, Mu Y, Gu W. Efficacy and Safety of Eldecalcitol for Osteoporosis: A Meta-Analysis of Randomized Controlled Trials. Front Endocrinol (Lausanne). 2022 Apr 19;13:854439.
- Matsumoto T, Takano T, Yamakido S, Takahashi F, Tsuji N. Comparison of the effects of eldecalcitol and alfacalcidol on bone and calcium metabolism. J Steroid Biochem Mol Biol. 2010 Jul;121(1-2):261-4.
- Cui, L., Xia, W., Yu, C. et al.Overview of the clinical efficacy and safety of eldecalcitol for the treatment of osteoporosis. Arch Osteoporos 2022;17:74.
